Dengue and malaria are two different diseases — but they share a striking common thread. Both are spread by mosquitoes. Both attack the blood directly: dengue triggers a dangerous drop in blood platelets that can cause internal bleeding, while malaria destroys red blood cells and leads to severe anaemia. In their most serious forms, both may require an urgent blood transfusion to save a life.
This is why World Blood Donor Day (14 June) and ASEAN Dengue Day (15 June) carry joint significance. Cities need safe blood supplies — and the governance systems that reduce the demand for them through prevention.
Both diseases also share the same urban logic: they thrive where drainage is poor, waste is unmanaged, and standing water accumulates unchecked. Where cities govern their environment well, both diseases retreat. Where governance slips, both advance. And when a city eliminates one, that same governance capacity becomes the foundation for fighting the next.
This article shares one city’s story across both diseases. Badulla, Sri Lanka — a compact hill city in Uva Province and a participant in the WHO South-East Asia Region Healthy Cities Network — sits within a country that this year marks a decade since receiving its WHO malaria-free certification. That national journey, and what it takes to sustain such gains, speaks directly to Badulla’s current work on dengue.
Part I · The Malaria Journey — A Century of Governance
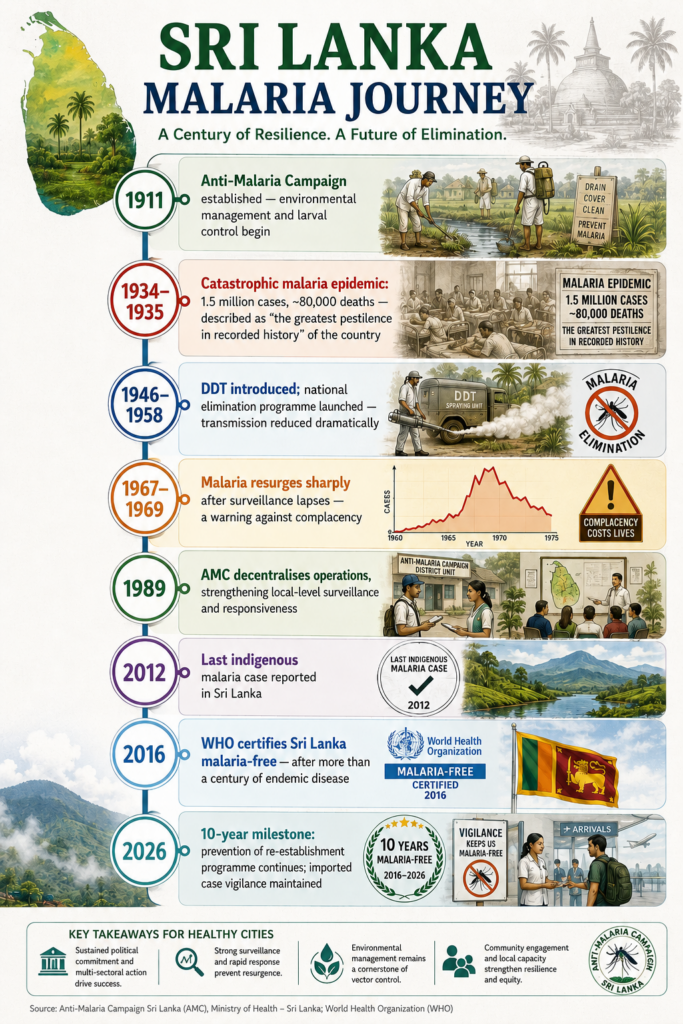
Sri Lanka marked a decade since receiving its WHO malaria-free certification in September 2016 — and fourteen years since the last reported indigenous case in 2012. For a country that endured malaria for centuries, including an outbreak in 1934–1935 that struck approximately 1.5 million people and caused nearly 80,000 deaths, this milestone represents one of the most consequential public health achievements in the region.
The journey was neither quick nor linear. Sri Lanka’s Anti-Malaria Campaign (AMC), established as far back as 1911, laid the institutional foundation through environmental management, larval control, and community outreach — long before modern insecticides existed. DDT was introduced in 1946, and a national elimination programme launched in 1958 dramatically reduced transmission. Yet when the programme’s momentum faltered in the 1960s, malaria resurged sharply between 1967 and 1969. History made its lesson clear: success is temporary when surveillance slips and political commitment wavers.
The AMC decentralised its operations in 1989 to strengthen local-level implementation and responsiveness — a structural governance decision that proved critical to building the consistent, granular surveillance needed to finally interrupt transmission. By 2012, indigenous cases had stopped entirely. Certification followed in 2016.
But elimination is not a finish line. Ten years on, Sri Lanka continues to face imported malaria cases — between 50 and 100 annually since 2013 — carried in by returning travellers and migrant workers from endemic neighbours including India and Myanmar. Competent mosquito vectors remain present across the country. In March 2026, the WHO Representative visited the AMC to reaffirm the shared commitment to prevention of re-establishment. The work continues through strengthened passive and active case surveillance, entomological monitoring, and prophylaxis for travellers to high-risk areas — all sustained by a multi-sector partnership involving the Ministry of Health, UN agencies, academic institutions, and international donors.
What Sustained Sri Lanka’s Malaria Elimination
- Over a century of institutional continuity through the Anti-Malaria Campaign (AMC)
- Decentralised, local-level surveillance and case investigation from 1989 onwards
- Multi-sector coordination: Ministry of Health, military, immigration, local councils, international donors
- Active and passive case detection systems maintained post-certification
- Entomological monitoring to track vector presence and any new species
- Prophylaxis provision and follow-up of imported cases from endemic neighbours
- WHO-supported integrated review of vector-borne diseases (2024) to strengthen defences further
Part II · The Dengue Challenge — Building upon Lessons Learnt
Badulla itself is a compact city of roughly 46,000 residents spread across just 10 square kilometres, set at 680 metres above sea level in Sri Lanka’s Uva Province — perpetually cloudy, cool, and wet. That climate shapes its dengue risk directly. Unlike hotter cities where heat dries standing water and accelerates waste decomposition, Badulla’s fog and persistent rain mean that blocked drains stay waterlogged longer, uncollected waste sits for extended periods, and water pooling in cracked or ageing tanks lingers. Dengue is listed as one of the municipality’s five top public health priorities alongside solid waste, food hygiene, child mortality, and nutrition.
The connection to Sri Lanka’s malaria story is not merely symbolic. The same governance principles that enabled malaria elimination — sustained local surveillance, integrated environmental management, community engagement, long-term political commitment — are precisely what Badulla’s Healthy Cities strategy is now applying to dengue. Rather than treating waste management and disease control as separate departmental concerns, the municipality has merged them into one strategy: fixing the environment is the health intervention.
Six community health assistants conduct year-round dengue inspections across all city divisions, feeding regular reports to the District Health Officer to enable early response before outbreaks escalate. Legal enforcement against illegal dumping was strengthened, signalling that sanitation is a civic obligation linked directly to public health. The city committed 3 million LKR to replacing deteriorating water tanks that had become hidden breeding sites, 1.3 million LKR to drain repair, and 1 million LKR to community cleaning programmes — each investment justified through its direct connection to vector control.
What Badulla Is Doing On Dengue
- Year-round inspections by 6 community health assistants across all city divisions
- Legal enforcement against illegal waste disposal — linking sanitation law to disease prevention
- 3 million LKR to replace deteriorating water tanks identified as mosquito breeding sites
- 1.3 million LKR for drain repair; 1 million LKR for community cleaning programmes
- Awareness outreach to schools, businesses, government offices, and community groups
- Emergency fumigation during confirmed high-prevalence periods
- Long-term WHO Healthy Cities commitment through 2030
Sri Lanka’s malaria journey showed that sustained vigilance — not a one-off campaign — is what produces lasting results. Badulla’s dengue plan is built on the same understanding. The Municipal Commissioner’s commitment to the WHO Healthy Cities programme through 2030 is not a programme announcement. It is an institutional decision to treat vector-borne disease prevention as a permanent function of city governance.
What This Tells Us
Badulla’s dual journey — from a country that once nearly lost to malaria, to a city now systematically preventing dengue — distils into four lessons that travel beyond Sri Lanka.
- Elimination is a governance achievement, not a medical event. Sri Lanka’s malaria-free status was built on over a century of institutional continuity, decentralised surveillance, and political commitment that did not waver even through civil conflict. The disease did not disappear because of a single intervention — it retreated because governance held.
- The same levers fight both diseases. Environmental management, local surveillance, community engagement, and integrated planning apply equally to malaria and dengue. A city that governs its sanitation and drainage well protects against both simultaneously.
- Success creates new vulnerability. Sri Lanka’s post-certification risk — declining clinical familiarity, imported cases, complacent surveillance — mirrors exactly what happened during the 1967–1969 resurgence. Badulla’s year-round inspection model is a direct response to this lesson: prevention must be continuous, not reactive.
- Community ownership is what makes governance durable. Cities like Khulna, Bangladesh — another WHO UGHW city where over 200 residents joined officials to clear mosquito breeding sites in Ward 30 in April 2025 — demonstrate that dengue control embedded in community practice outlasts any government-run campaign. Badulla’s awareness outreach and Khulna’s co-designed cleanups point toward the same conclusion: residents are not the audience for health programmes. They are co-deliverers.
- Blood supply is part of the equation. Both dengue and malaria can require urgent transfusion in severe cases. Supporting voluntary blood donation — reinforced every 14 June — is a concrete preparedness step that sits alongside, not separate from, prevention and governance work.
As Dr Pandav put it on World Malaria Day 2026: the fight does not end with elimination — it must be sustained to protect the gains achieved. Badulla, and cities like it across the region, are where that sustaining work happens every day.
Suchinda Phaisomboon, Regional Communications Officer
REFERENCES
Badulla Municipal Council. (2024). City Health Action Plan — WHO SEAR Healthy Cities Initiative.
WHO Bangladesh. (September 2025). Fighting dengue together: how community engagement is transforming health in Khulna City. Retrieved from https://www.who.int/news-room/feature-stories/detail/fighting-dengue-together–how-community-engagement-is-transforming-health-in-khulna-city–bangladesh
WHO Sri Lanka. (April 2026). “Driven to End Malaria”: Ten years of success for Sri Lanka. Retrieved from https://www.who.int/srilanka/news/detail/24-04-2026-driven-to-end-malaria—ten-years-of-success-for-sri-lanka
WHO. (2025). Dengue and severe dengue — Fact Sheet. Retrieved from https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue
WHO. (October 2024). Global Strategic Preparedness and Response Plan for Dengue. Retrieved from https://www.who.int/publications/m/item/global-strategic-preparedness–readiness-and-response-plan-for-dengue-and-other-aedes-borne-arboviruses
WHO. (2024). World Malaria Report 2024. Retrieved from https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2024
WHO. (September 2016). WHO certifies Sri Lanka malaria-free. Retrieved from https://www.who.int/southeastasia/news/detail/05-09-2016-who-certifies-sri-lanka-malaria-free
WHO. (2023). Towards a malaria-free world: elimination of malaria and prevention of re-establishment in Sri Lanka. Retrieved from https://www.who.int/publications/b/72366
WHO–UN-Habitat. (2021). Global framework for the response to malaria in urban areas. Retrieved from https://www.who.int/publications/i/item/9789240061781
